To the Editor:
Chin et al1 should be commended for their very interesting special article on
abdominal wall blocks. Regarding the de scribed posterolateral approaches, we agree that quadratus lumborum (QL) type 12 and transversalis fascia (TF) block3 appear similar. The authors claim that, in both techniques, the injection spread occurs into the plane between the transversus abdominis muscle (TAM) and the TF. We wondered if we would not have to rename the anatomical topography of injections originally de scribed and labeled.
After informed and signed consent, we studied the spread of bilateral analgesic QL1 or TF block in 7 patients, scheduled for trauma or surgical-purposes computed tomography. We demonstrated in all cases a predominant spread of contrast media in the retroperitoneal space (Figs. 1A–C).
Weassert that in the ultrasound image the local anesthetic (LA) spread over the in ner surface of the TAM in QL1 and TF blocks corresponds to an injection deep to the TF (ie, in the retroperitoneal posterior pararenal space [PPS]). Likewise, we argue that the spread of contrast media observed
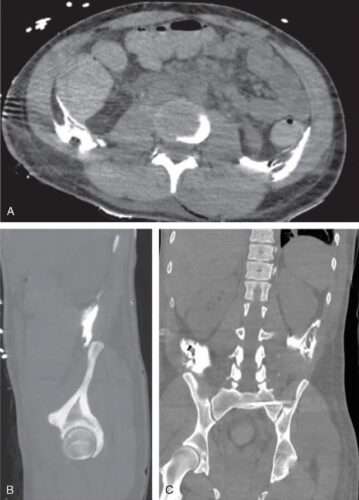
FIGURE 1. Axial (A), right-side coronal (B), and sagittal (C) computed tomography scan views after bilateral QL1 block. The images highlight the spread of contrast media in the retroperitoneal PPS and the absence of spread in the retrofascial muscular spaces.
along the QL in the posterior approach of Carney et al4 was over the inner surface of the muscles in the retroperitoneum. The confusion may come from terminology of the fascial layers of the posterior abdominal wall. As reported from the reviewof Anson et al,5 the TF is separated from the perito neum by a variable amount of connective tissue. It is a layer of loose connective tissueeasily separated from the TF inpatients. It has some tensile strength and has frequently been mistaken for the TF in cadavers. In accordance with Terminologica Anatomica, TF is the innermost layer of the parietal fascia of the abdomen. Hence, TF is an additional term for the innermost epimysium. No separate deep investing fascia exists.6 The retroperitoneal space liesposteriorly to the parietal peritoneum and anteriorly to the TF.7 The subcostal, iliohypogastric, and ilioinguinal nerves run within behind the kidney downward and laterally in front of the QL and penetrate the TAM and then the TA plane. In the lumbar area, the posterior portion of the retroperitoneal space is the PPS.8 The adipose tissue layer is markedly thickened from kidney downward anterior to the QL, psoas, and iliac muscles fascia. The PPS is limited anteriorly by the posterior renal fascia, opens laterally toward the flank, and merges inferiorly with retro peritoneal tissues of the iliac fossa. Conse quently, the likely mechanism of inadvertent femoral nerve block after abdominal wall blocks 9 is related to an LA solution spreading inferiorly from the pararenal fat to the iliopsoas fascia and to the femoral nerve. Behind the TF is the retrofascial space containing the posterior abdominal wall, nerves, lymphatics, areolar tissue, and QL, psoas, and iliacus muscles.10 This retrofascial space is divided in 3 compartments by the layers of the thoracolumbar fascia: the psoas compart ment, the lumbar region, and the iliac area.
In ultrasound-guided posterolateral abdominal blocks, 3 main distinct patterns of injectate spreads should be visualized in the different anatomical compartments. In the QL3 block, in which LA is injected between the QL and the psoas muscle,11 the spread is confined in the psoas com partment described by Chayen et al.12 In QL 2 blocks, the LA solution, injected posterior to the QL in the lumbar interfascial triangle, runs in the muscular planes of the lumbar region.13 Finally, in both QL1 and FT blocks, the LA solution spreads deep to FTwithin the PPS.
The authors declare no conflict of interest.
1. Chin KJ, McDonnell JG, Carvalho B, Sharkey
A, Pawa A,GadsdenJ. Essentials of our current
understanding: abdominal wall blocks.
Reg Anesth Pain Med. 2017;42:133–183.
2. Blanco R, McDonnell JG. Optimal point of
injection: the quadratus lumborum type I and II
blocks. 2013. Available at: http://www.
articlescom/ANA/forums/post/1550aspx.
Accessed December 25, 2016.
3. Hebbard PD. Transversalis fascia plane block, a
novel ultrasound-guided abdominal wall nerve
block. Can J Anaesth. 2009;56:618–620.
4. Carney J, Finnerty O, Rauf J, Bergin D, Laffey
JG, Mc Donnell JG. Studies on the spread of
local anaesthetic solution in transversus
abdominis plane blocks. Anaesthesia.2011;66:
1023–1030.
5. Anson BJ, McVay CB. Surgical Anatomy.5th
ed. Philadelphia: WB Saunders Co; 1971.
6. Skandalakis PN, Zoras O, Skandalakis JE,
Mirilas P. Transversalis, endoabdominal,
endothoracic fascia: who’s who? Am Surg.
2006;72:16–18.
7. Mirilas P, Skandalakis JE. Surgical anatomy of
the retroperitoneal spaces—part I:
embryogenesis and anatomy. Am Surg.2009;
75:1091–1097.
8. Mirilas P, Skandalakis JE. Surgical anatomy of
the retroperitoneal spaces—part II: the
architecture of the retroperitoneal space.
AmSurg.2010;76:33–42.
9. Wikner M. Unexpected motor weakness
following quadratus lumborum block for
gynaecological laparoscopy. Anaesthesia.2017;
72:230–232.
10. Weinberg K, Telegrafi S. The retroperitoneum.
In: Hagen-Ansert SL, ed. Textbook of
Diagnostic Sonography. 7th ed. Atlanta, GA:
Elsevier Health Sciences; 2013.
11. Børglum J, Jensen K, Moriggl B, et al.
Ultrasound-guided transmuscular quadratus
lumborum blockade. Br J Anaesth.2013;111
(eLetters Supplement). DOI: https://doi.org/10.
1093/bja/el_9919.
12. Chayen D, Nathan H, Chayen M. The psoas
compartment block. Anesthesiology.1976;45:
95–99.
13. Blanco R, Ansari T, Riad W, Shetty N.
Quadratus lumborum block versus transversus
abdominis plane block for postoperative pain
after cesarean delivery: a randomized controlled
trial. Reg Anesth Pain Med. 2016;41:757–762.