Background and Objectives: This cadaveric study investigated the anatomic relationships of the articular branches of the suprascapular (SN), axillary (AN), and lateral pectoral nerves (LPN), which are potential targets for shoulder analgesia.
Methods: Sixteen embalmed cadavers and 1 unembalmed cadaver, including 33 shoulders total, were dissected. Following dissections, fluoroscopic images were taken to propose an anatomical landmark to be used in shoulder articular branch blockade.
Results: Thirty-three shoulders from 17 total cadavers were studied. In a series of 16 shoulders, 16 (100%) of 16 had an intact SN branch innervating the posterior head of the humerus and shoulder capsule. Suprascapular sensory branches coursed laterally from the spinoglenoid notch then toward the glenohumeral joint capsule posteriorly. Axillary nerve articular branches innervated the posterolateral head of the humerus and shoulder capsule in the same 16 (100%) of 16 shoulders. The AN gave branches ascending circumferentially from the quadrangular space to the posterolateral humerus, deep to the deltoid, and inserting at the inferior portion of the posterior joint capsule. In 4 previously dissected and 17 distinct shoulders, intact LPNs could be identified in 14 (67%) of 21 specimens. Of these, 12 (86%) of 14 had articular branches innervating the anterior shoulder joint, and 14 (100%) of 14 LPN articular branches were adjacent to acromial branches of the thoracoacromial blood vessels over the superior aspect of the coracoid process.
Conclusions: Articular branches from the SN, AN, and LPN were identified. Articular branches of the SN and AN insert into the capsule overlying the glenohumeral joint posteriorly. Articular branches of the LPN exist and innervate a portion of the anterior shoulder joint.
(Reg Anesth Pain Med 2017;42: 00–00)
Pain of the shoulder, including the glenohumeral joint (GHJ), acromioclavicular joint (ACJ), and rotator cuff, is prevalent and responsible for significant health burden.1–4 Innervation of the GHJ can be divided into anterior and posterior innervation from articular branches of the suprascapular nerve (SN) (posterior-lateral), axillary nerve (AN) (anterior-lateral, inferior, and posterior-lateral), and lateral pectoral nerve (LPN) (anteriorsuperior).5,6 These nerves also provide substantial motor innervation. Considering the burden of shoulder pain worldwide, the potential to provide nerve blocks and neuroablative treatments with minimal weakness warrants serious consideration.6–9
The LPN has gained attention for chest wall and postmastectomy pain10 but is underrecognized as a contributor to shoulder structures. Anatomical studies describe the LPN originating from C5–7 nerve roots, supplying innervation to the skin over
the subacromial bursa,5,11 muscular innervation of the pectoralis major and deltoid muscles,5 and intra-articular innervation to the ACJ3,4 and anterior GHJ.5,6,11 Innervation of the ACJ and GHJ via articular branches of the LPN has potential for peripheral nerve blockade,5,6 similar to AN and SN blocks.5–7
The AN originates from the posterior cord of the brachial plexus, dividing into anterior and posterior branches in the quadrangular space.12 The nerve then innervates the deltoid muscle, teres minor muscle, shoulder joint capsule, and inferior GHJ, with its superior-lateral brachial cutaneous branch providing sensation over the deltoid muscle.12,13 The AN is compelling for providing shoulder analgesia as demonstrated during preoperative blockade for upper-extremity surgeries.13
Originating from nerve roots C5–6, the SN branches off the superior trunk of the brachial plexus, coursing through the posterior triangle of the neck, and enters the suprascapular notch and spinoglenoid notch.14 The nerve innervates the supraspinatus muscle and infraspinatus muscle and provides sensory input from the lateral upper extremity, GHJ, ACJ, subacromial bursa, coracohumeral ligament, and coracoacromial ligaments.15
The SN is established as a target for shoulder analgesia in clinical practice.7,9,16,17
This study investigated the anatomic course of the SN, AN, and LPN to the GHJ in cadavers. We aimed to determine the location of terminal sensory articular branches of the shoulder and describe associations with bone, soft tissue, and vascular landmarks. Enhanced knowledge of terminal sensory nerve branches could provide interventional targets for joint and ligament pain, with low risk of muscle weakness.
Part 1: Literature Review A thorough literature review was performed using the filter marked “humans” in the PubMed database. To facilitate consistency, the key words suprascapular/axillary/lateral pectoral nerve, articular branch, and anatomy were used in various combinations to assist in review. After using these search criteria, 23, 22, and 7 articles, respectively, were found and evaluated. Three articles for each nerve were deemed to be relevant to the purpose of this study and are discussed in Table 1.
Part 2: Cadaveric Dissection In the cadaveric dissection portion of this study, 16 embalmed cadavers and 1 unembalmed cadaver, representing 33 usable shoulder specimens, were dissected to evaluate the anatomic course of the articular branches of LPN, SN, and AN. The care, handling, dissection, and radiographic evaluation of all cadavers were completed in compliance with the rules and regulations of the State Anatomical Board of the State of Texas and the policies, procedures, and ethical guidelines of The University of Texas Health Science Center at San Antonio Department of Cell Systems
SN
AN
LPN
and Anatomy and the body donation program. Thorough dissections were performed to confirm and add to the limited prior cadaveric studies5,6,11 investigating the articular branches of the GHJ. The cadaver was placed in prone (SN and AN) or supine (LPN) positioning, with both shoulders in internal rotation. All cadaver specimens were embalmed while in upper-extremity internal rotation, preventing full passive range of motion of the shoulder into anatomical external rotation.
Suprascapular Nerve Sixteen shoulders (14 embalmed and 2 unembalmed) from 8 cadavers were examined for study of the SN. A coronal incision
was made along the superior border of the clavicle extending from its proximal origin to the first one-third of the shaft of the humerus. A second incision was made vertically extending from the proximal point of the first incision until halfway through the
thorax, passing the inferior scapular angle. The third and final incision began at the inferior edge of the second incision, extending laterally to the midaxillary line and then connecting to the distal point of the first incision on the humeral shaft. The skin and superficial adipose layers were removed, exposing the entire scapula, axilla, and deltoid muscle.
The spine and medial border of the scapula were then palpated, and an incision was made along these 2 borders.
The infraspinatus muscle was reflected toward its origin in the infraspinous fossa, with care taken not to disturb the neurovascular bundle innervating the infraspinatus muscle. The SN and suprascapular artery and vein were identified exiting the spinoglenoid notch.
Axillary Nerve
Sixteen shoulders (14 embalmed and 2 unembalmed) from the same 8 cadavers used for the SN dissections were examined for study of the AN. A coronal incision was made along the distal tip of the acromion through one-third of the shaft of the humerus. The skin and superficial adipose layers were removed. The quandrangular space was identified, and excess adipose removed. The investigator exposed the AN and posterior circumflex humeral artery and vein exiting the quandrangular space. An incision was made along the superior origin of the deltoid muscle and was carefully reflected inferiorly without damaging the fascia between the deltoid muscle and head of the humerus.
Lateral Pectoral Nerve
Twenty-one shoulders, all embalmed, from 11 cadavers were examined for study of the LPN. Four shoulders (2 cadavers) were shared from the SN/AN group, whereas the remaining 17 shoulders were supplied from 9 separate cadavers. Given increased delicacy of the LPN compared with SN and AN, more specimens were studied for LPN. With the cadaver supine, a coronal incision was made along the anterior aspect of the clavicle, beginning with its most proximal point and ending at the first one-third of
the shaft of the humerus. A second incision was made vertically along the sternum, extending halfway down the thorax. Starting at the distal point of the second incision, a third transverse incision was made to extend laterally to the distal point of the first incision at the shaft of the humerus. The skin and superficial adipose layers were removed to expose the pectoralis major and minor muscles, deltoid muscle, clavicle, and axilla. An incision was made along the sternum and inferior pectoralis major muscle to reflect the muscle superiorly, careful not to disturb the underlying structures. The medial pectoral nerve was identified piercing both pectoralis major and minor
muscles, and then the LPN was identified piercing pectoralis major muscle. The LPN was traced back to its origin at the lateral cord of the brachial plexus.
Part 3: Fluoroscopy
After dissections were completed, the investigators selected a cadaveric shoulder to be evaluated under fluoroscopy. Under fluoroscopy, anatomical landmarks, including the coracoid, acromion, humeral head, humeral neck, and glenoid fossa, were identified for needle placement. An 18-gauge aluminum wire was placed on the specimen, tracing the pathway of the SN, AN, and LPN to demonstrate relationships with nearby anatomic structures. The fluoroscopy system was positioned in an anterior-posterior (LPN) or posterior-anterior (SN and AN) direction without any initial angular deviation in the medial, lateral, caudal, or cephalad direction. A series of fluoroscopic films were taken starting directly above the prone (SN and AN) or supine (LPN) cadaver (0 degrees) and proceeding at 5-degree increments until directly lateral to the humerus (90 degrees).
Cadaveric Dissection
Suprascapular Nerve
The SN was visualized in the spinoglenoid notch and identified innervating the supraspinatus and infraspinatus muscle. The main trunk of the SN gave articular branches superiorly and inferiorly to the spinoglenoid notch. Superiorly, these articular
branches were seen along the supraspinous fossa of the spine of the scapula, coursing laterally toward the posterior GHJ and head of the humerus in all specimens. The nerves were then seen piercing the fascia overlying the head of the humerus (Figs. 1A and 2A). After the sensory nerves branched from the main trunk of SN superior to the spinoglenoid notch, no motor branches, other than the proximal motor branch innervating the supraspinatus muscle, were visualized. The SN displayed these anatomical pathways in 16 (100%) of 16 specimens. As the SN passed inferiorly through the spinoglenoid notch, the main trunk proceeded medially to innervate the infraspinatus muscle, whereas the articular branches coursed laterally in the infraspinous fossa of the spine of the scapula toward the posterior inferior GHJ and head of the humerus. Terminal articular nerves were seen piercing the fascia overlying the head of the humerus in 100% of the specimens.
The suprascapular artery and vein were identified passing through the spinoglenoid notch. However, branches of the artery and vein did not appear to be associated with the terminal articular sensory branches described in the supraspinous and infraspinous
fossae of the spine of the scapula. Rather, these vessels appeared to accompany the motor branches innervating the supraspinatus and infraspinatus mm.
Axillary Nerve
After the AN was identified exiting the quadrangular space, its branches were followed until termination. Two motor branches came off the main trunk of the AN immediately distal to the quadrangular space and innervated the deltoid and teres minor muscle. The teres minor muscle branch appeared to have only motor innervation with all terminal branches piercing the muscle. The branch innervating the deltoid muscle coursed laterally around the head of the humerus, with the larger branch piercing the deltoid muscle adjacent to the lateral aspect of the humerus. Just proximally to the point of piercing the deltoid muscle, the larger branch gave off multiple smaller articular branches medially back toward the head of the humerus to innervate the posterior and lateral overlying fascia (Figs. 1B and 2B). These anatomic pathways were observed in 16 (100%) of 16 specimens.
The posterior humeral circumflex artery and vein were identified in the quadrangular space next to the main trunk of the AN. However, the artery and vein did not accompany terminal articulating sensory branches in any of the specimens.
Lateral Pectoral Nerve
Twenty-one intact shoulder girdles were evaluated for suitability of dissection. In 14 of these, tissue integrity was amenable to identification of the LPN. In 12 (86%) of these 14 shoulder
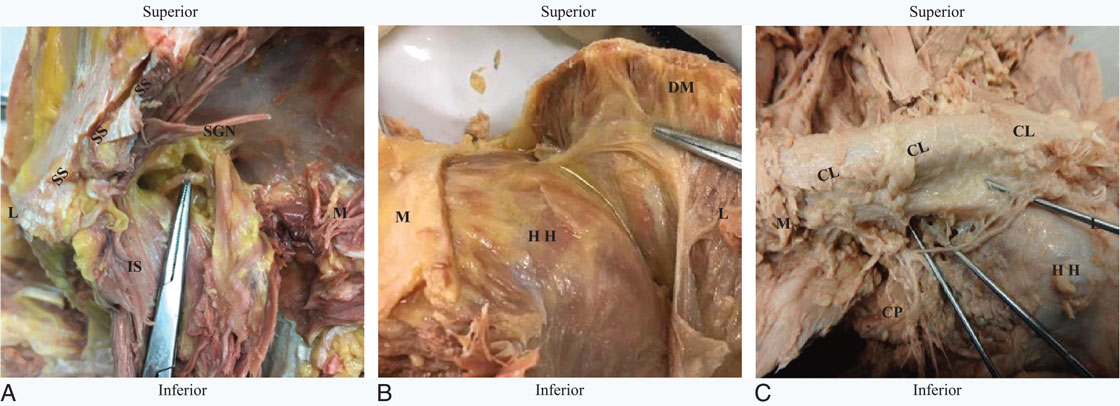
FIGURE 1. Cadaver photographs of SN (A), AN (B), LPN (C). A, Left shoulder is seen in prone positioning. The sensory articular branch of SN (lifted by probe) exits the main trunk of SN (seen on reflected IS) and travels laterally toward GHJ. B, Right shoulder is seen in prone positioning. The sensory articular branch of AN (probe) seen deep to DM (reflected), traveling in fascia to return medially toward HH. C, Left shoulder is seen in supine positioning. The sensory articular branches of LPN (probes) travel laterally to provide sensation to anterior
girdles, an intact LPN with articular branches crossed the coracoclavicular ligament, pierced the coracoacromial ligament, and entered the anterior superior GHJ (Figs. 1C and 2C). The remaining had an intact LPN, but distal anatomic course could not be determined because of loss of cadaveric integrity. These LPN articular branches were adjacent and generally superior to the acromial branch of the thoracoacromial artery in 14 (100%) of 14 cases. A muscular branch from the LPN to the deltoid muscle was identified in 3 (21%) of 14 cases.
Fluoroscopy
Suprascapular Nerve
Under fluoroscopy, a specimen was evaluated, and the posterior acromion, glenoid fossa, humeral head, and humeral neck were successfully identified. The aluminum wire, imitating the course of the SN, was easily visualized in the fluoroscopy views.
The anatomic structures and aluminum wire were clearly visible and easily identified in views from 0 to 60 degrees without any cephalad, caudad, superior, or inferior deviation (Fig. 3A). Beyond 60 degrees, these structures and aluminum wire were difficult to identify because of increased fluid penetration of the surrounding soft tissue structures.
Axillary Nerve
For the AN, the posterior acromion, glenoid fossa, humeral head, and humeral neck were identified under fluoroscopy in the same manner as identified in the previous section. An aluminum wire was placed over the course of the AN in order to identify it in relation to nearby anatomic structures. Again, the aluminum wire and anatomic structures were easily identified in 0- to 60-degree views (Fig. 3B) before the increased fluid penetration of higher angles interfered with visualization, as in the SN.
Lateral Pectoral Nerve
After the dissection and investigation of the anatomical course of the LPN, investigators evaluated a cadaveric shoulder in the anterior view to determine if the coracoid process could be appropriately identified under fluoroscopy, allowing it to be an anatomic landmark for articular LPN identification. The cadaveric shoulder was placed in the supine position, with the shoulder in internal rotation, for reasons mentioned previously. This was similar to an anterior approach to the SN as described by Ebraheim et al.18 The coracoid process and aluminum wire were easily identified in 0- to 60-degree views (Fig. 3C). Beyond these views, at increasing angles, structures became difficult to identify because of increased fluid collections and poor penetration. capsule over the HH. SS, suprascapular spine; SGN, spinoglenoid notch; IS, infraspinatus muscle; DM, deltoid muscle; HH, humeral head; CL, clavicle; L, lateral; M, medial; CP, coracoid process; AC, acromion process.
Suprascapular Nerve
Prior studies of the SN identified terminal articular branches to the coracoclavicular and coracohumeral ligaments,6 ACJ,6,18 subacromial bursa,6,18 and posterior shoulder capsule.6,19 These studies focused on superior and proximal aspects of the SN with identification along the coracoid and acromion anatomic regions. In comparison, the investigators of this study identified the course of the SN as it passes through the spinoglenoid notch and continues to give terminal articular branches to the joint in all of our specimens. This study elucidates previously undescribed anatomy of the SN as its articular branches course laterally in the supraspinous and infraspinous fossae of the spine of the scapula to innervate the posterior GHJ, posterior shoulder capsule, subacromial bursa, and posterior fascia of the head and neck of the humerus. These terminal articular branches do not contain motor fibers and are regionally distinct from their proximal mixed motor-sensory trunk as it exits the spinoglenoid notch.
Anatomic descriptions of terminal sensory nerves and their relation to nearby anatomic landmarks and vessels have not been previously described. The SN terminal sensory branches provide innervation to the posterior shoulder joint without innervating nearby musculature.
The SN terminal sensory branches are in a region clearly distinct from motor fibers, as seen in zones 2A and 3A in Figure 4. Procedures in this area may avoid damage to the mixed motor-sensory and pure motor branches as shown in zone 1A in Figure 4. The nearby anatomic landmarks of the
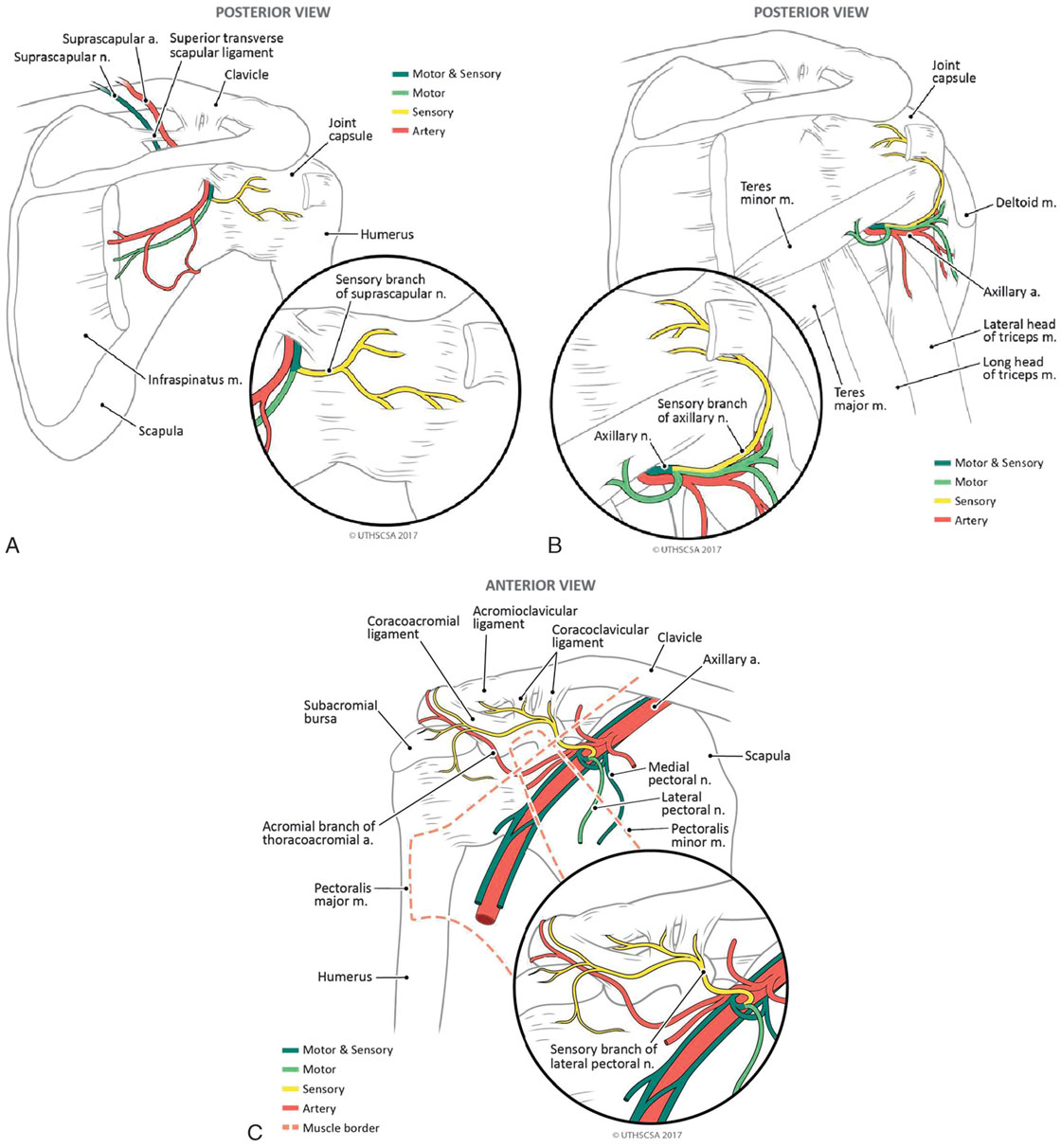
FIGURE 2. Medical illustrations depicting the anatomic course of SN (A), AN (B), and LPN (C). A, The SN exiting the spinoglenoid notch. A motor branch immediately innervates infraspinatus, whereas the sensory branch travels laterally in the infraspinous fossa to innervate the humeral head and shoulder capsule. B, The AN exiting the quadrangular space, wrapping laterally to innervate the deltoid muscle and then continuing to provide pure sensory innervation to the posterior-lateral humeral head and shoulder capsule. C, The LPN branching from the upper trunk of the brachial plexus to innervate the pectoralis major muscle with a motor branch. A pure sensory branch of LPN then continues superior to the acromial branch of the thoracoacromial artery to innervate the anterior superior GHJ and coracoacromial ligament.
glenoid fossa, acromion, humeral head, and humeral neck allow for reliable identification of these zones.
Axillary Nerve
This study identified terminal articular branches of the AN in all 16 shoulder specimens studied. In all specimens, the AN gave terminal articular branches distal to teres minor and deltoid motor branches. These terminal articular branches were oriented in an
inferior-superior (teres minor muscle) or lateral-medial (deltoid muscle) direction to innervate the fascia of the humeral head and neck, inferior GHJ, and inferior-posterior shoulder joint capsule in all specimens. This anatomic pattern is similar to previous
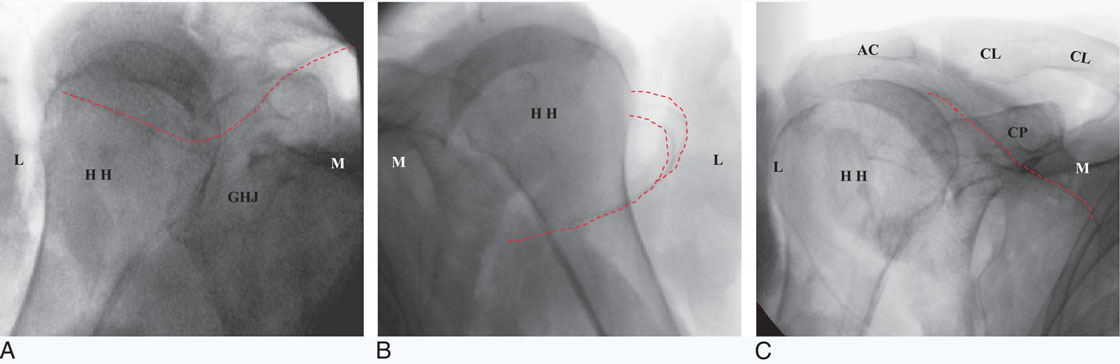
FIGURE 3. Fluoroscopy photographs of SN (A), AN (B), and LPN (C). A, Left shoulder, prone positioning. The sensory articular branches of SN travel laterally after exiting spinoglenoid notch and innervating the posterior shoulder capsule. The HH and GHJ are clearly seen under fluoroscopy. B, Right shoulder, prone positioning. The sensory articular branches of AN branch from the main AN trunk after providing motor innervation to the deltoid and then travel medially toward the HH. HH is clearly seen under fluoroscopy. C, Right shoulder, supine positioning. The LPN articular branches travel laterally inferior to the AC and CL and lateral to CP. CP, CL, AC, and HH are clearly seen under fluoroscopy. HH, humeral head; CL, clavicle; L, lateral; M, medial; CP, coracoid process; AC, acromion process.
studies,20,21 but with more consistency. In addition, this study evaluated motor branches of the AN and their relationship to the pure sensory articular branches. In all specimens, the terminal articular branches provided pure sensory innervation and did not have any motor contributions. These sensory fibers were in clearly distinct anatomic regions, zones 2A and 3A, compared with their proximal motor counterparts, zones 1B and 2B (Fig. 4). This study confirmed the existence of these terminal sensory
articular branches of AN. The investigation of the anatomic relationship between sensory articular branches and motor branches of the AN was previously not described. The glenoid fossa, acromion, humeral head, and humeral neck would be ideal anatomic landmarks in fluoroscopy examinations as demonstrated in this study.
Lateral Pectoral Nerve
The anatomic course of the articular branches described in this study was similar to that in the study of Aszmann et al6 and is summarized in Table 1. Further studies could focus on ability to identify acromial and possibly deltoid branches of the thoracoacromial artery with ultrasound and using those vessels as an anatomic reference to find and block the articular branches of LPN to the shoulder joint. The LPN articular branch appears to have a branch to the clavicle, acromion joint, subacromial bursa, and occasional muscular branch to the deltoid. The LPN may have another branch, often separate from the articular branch, innervating the subclavius muscle. Statistical analysis of these LPN branches and variants was beyond the scope of this study.
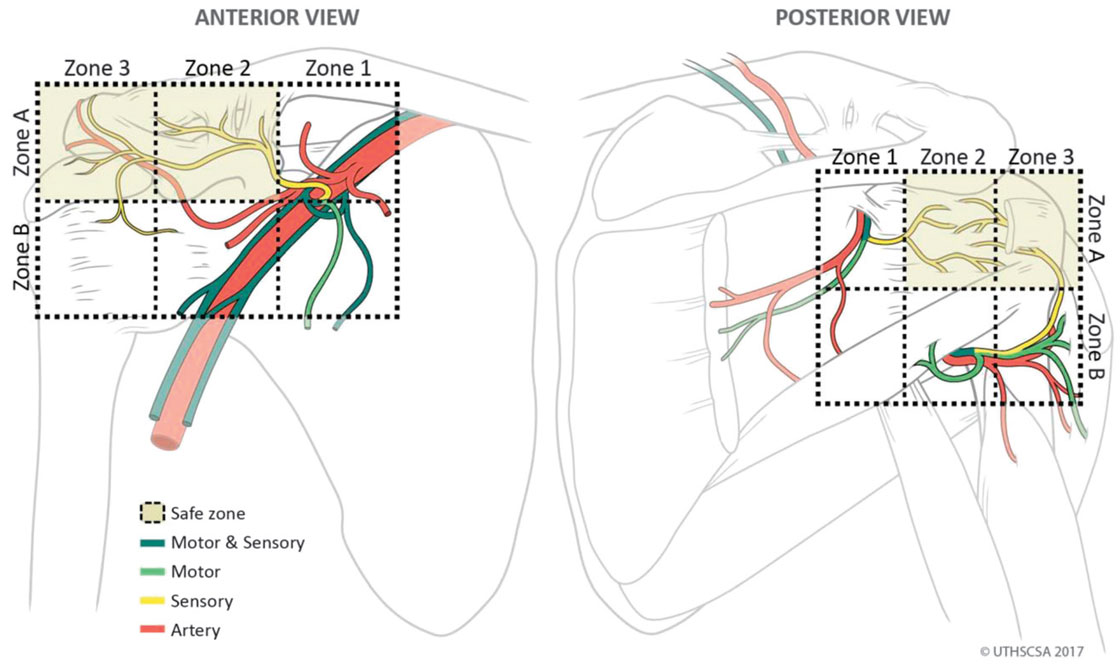
FIGURE 4. Medical illustrations depicting anatomic safe zones. Anterior view: zones 1 and 2 are bisected by the proximal end of the coracoid process. Zones 2 and 3 are bisected by the distal end of the coracoid process. Zones A and B are bisected by the inferior border of the coracoid process. Possible safe zones for sensory branch intervention are 2A and 3A. Posterior view: zones 1 and 2 are bisected by the GHJ.
Zones 2 and 3 are bisected by the medial-lateral plane of the humeral head. Zones A and B are bisected by the inferior pole of the GHJ and the surgical head of the humerus. Zones 2A and 3A are possible safe areas for sensory branch intervention.
The LPN articular branches in the anterior view are located in zones 2A and 3A as seen in Figure 4. Relevant landmarks are the acromion, coracoid process, GHJ, and acromial branch of thoracoacromial artery. In agreement with findings by Nam et al,5 the superior and distal aspect of the coracoid process appears to be a reasonable area to target the pure sensory portions of the LPN.
CONCLUSIONS
This cadaveric study confirmed prior studies’ results, which showed existence of SN, AN, and LPN articular branches. Suprascapular nerve sends additional articular branches posteriorly from a medial-lateral direction over the head of the humerus. Axillary nerve posteriorly sends articular branches from an inferiorsuperior and lateral medial direction. The LPN branches course in a superior-lateral direction adjacent to thoracoacromial vessels across the superior aspect of the coracoid process and then descends into the anterior-superior GHJ. Limitations to this study include small sample size and diminished tissue integrity in a few specimens (LPN group). Larger cadaveric studies investigating the full length of the nerves’ origin, variations, and commonality of branches to the subacromial region, deltoid muscle, ACJ, and GHJ should be undertaken. Validation and clinical prospective study are needed to establish the precision, safety, and effectiveness of SN, AN, and LPN articular blockade for shoulder pain.
ACKNOWLEDGMENTS
The authors thank Robert Chalk and the Anatomical Services staff of the Body Donation Program of the Department of Cell Systems and Anatomy and the Anesthesia Department for their continued support and assistance with providing materials and
staff for assistance of this study. The authors also thank the individuals who donate their bodies and tissues for the advancement of education and research.
REFERENCES
1. Andrews JR. Diagnosis and treatment of chronic painful shoulder: review of nonsurgical interventions. Arthroscopy. 2005;21:333–347.
2. Adey-Wakeling Z, Arima H, Crotty M, et al. Incidence and associations of hemiplegic shoulder pain poststroke: prospective population-based study. Arch Phys Med Rehabil. 2015;96:241–247.
3. Silvestri J. Effects of chronic shoulder pain on quality of life and occupational engagement in the population with chronic spinal cord injury: preparing for the best outcomes with occupational therapy. Disabil Rehabil. 2017;39:82–90.
4. Van der Windt D, Koes BT, de Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis. 1995;54:959–964.
5. Nam YS, Panchal K, Kim IB, Ji JH, Park MG, Park SR. Anatomical study of the articular branch of the lateral pectoral nerve to the shoulder joint. Knee Surg Sports Traumatol Arthrosc. 2016;24:3820–3827.
6. Aszmann OC, Dellon AL, Birely BT, McFarland EG. Innervation of the human shoulder joint and its implications for surgery. Clin Orthop Relat Res. 1996;330:202–207.
7. Klç Z, Filiz MB, Çakr T, Toraman NF. Addition of suprascapular nerve block to a physical therapy program produces an extra benefit to adhesive capsulitis: a randomized controlled trial. Am J Phys Med Rehabil. 2015; 94:912–920.
8. Kim JS, Nahm FS, Choi EJ, Lee PB, Lee GY. Pulsed radiofrequency lesioning of the axillary and suprascapular nerve in calcific tendinitis. Korean J Pain. 2012;25:60–64.
9. Tran DQ, Elgueta MF, Aliste J, Finlayson RJ. Diaphragm-sparing nerve blocks for shoulder surgery. Reg Anesth Pain Med. 2017; 42:32–38.
10. Bouzinac A, Tournier JJ, Delbos A, Bérot JE. Interest of ultrasound-guided lateral pectoral nerve block associated with paravertebral block for complete mastectomy pain management [in French. Ann Fr Anesth Reanim. 2014;33:548–550.
11. Akita K, Kawashima T, Shimokawa T, Sato K, Sato T. Cutaneous nerve to the subacromial region originating from the lateral pectoral nerve. Ann Anat. 2002;184:15–19.
12. Gurushantappa PK, Kuppasad S. Anatomy of axillary nerve and its clinical importance: a cadaveric study. J Clin Diagn Res. 2015;9: AC13–AC17.
13. Ball CM, Steger T, Galatz LM, Yamaguchi K. The posterior branch of the axillary nerve: an anatomic study. J Bone Joint Surg Am. 2003;85-A: 1497–1501.
14. Yang HJ, Gil YC, Jin JD, Ahn SV, Lee HY. Topographical anatomy of the suprascapular nerve and vessels at the suprascapular notch. Clin Anat. 2012;25:359–365.
15. Cummings CA, Messer TM, Nuber GW. Suprascapular nerve entrapment. J Bone Joint Surg Am. 2000;82:415–424.
16. Mortada MA, Ezzeldin N, Abbas SF, Ammar HA, Salama NA. Multiple versus single ultrasound guided suprascapular nerve block in treatment of frozen shoulder in diabetic patients. J Back Musculoskelet Rehabil. 2017;30:537–542.
17. Chan CW, Peng PW. Suprascapular nerve block: a narrative review. Reg Anesth Pain Med. 2011;36:358–373.
18. Ebraheim NA, Whitehead JL, Alla SR, et al. The suprascapular nerve and its articular branch to the acromioclavicular joint: an anatomic study. J Shoulder Elbow Surg. 2011;20:e13–e17.
19. Vorster W, Lange CP, Briët RJ, et al. The sensory branch distribution of the suprascapular nerve: an anatomic study. J Shoulder Elbow Surg. 2008;17:500–502.
20. Gelber PE, Reina F, Monllau JC, Yema P, Rodriguez A, Caceres E. Innervation patterns of the inferior glenohumeral ligament: anatomical and biomechanical relevance. Clin Anat. 2006;19:304–311.
21. Nasu H, Nimura A, Yamaguchi K, Akita K. Distribution of the axillary nerve to the subacromial bursa and the area around the long head of the biceps tendon. Knee Surg Sports Traumatol Arthrosc. 2015;23: 2651–2657.